Abdominal Compartment syndromE IN
polytrauma
L. Pleva, *J. Mayzlík, M. Šír
Trauma Centre, University Hospital Ostrava, *Clinic of Surgery, University Hospital Ostrava
Summary
Authors
inform about the group of 8 patients with abdominal compartment syndrome
(ACS) occurred as a complication in large blunt injury of abdominal
cavity. To the ACS diagnose, the measurement of intracystic pressure is
used routinely, whose values correlate fully with values of intraabdominal
pressure (IAP). In case of increasing values of IAP over 25 mm Hg with
positive clinical signs of ACS, authors indicate decompression laparotomy
with temporary closing of abdominal cavity by sterile plastic foil or
Ethizip. Preventive temporary laparostomy is recommended also in serious
injuries of abdominal cavity in patients threatened by fatal haemorrhage,
treated by the method of staged laparotomy with tamponade of abdominal
cavity and with massive blood and volume resuscitation.
Key words - blunt abdominal trauma, abdominal compartment syndrome, intraabdominal pressure, laparostomy.
Introduction
Abdominal
compartment syndrome (ACS) develops on the basis of increased
intraabdominal pressure (AP), with its pathophysiological consequences
manifesting all over the organism. After injuries, mostly in case of
serious abdominal injuries with massive intraabdominal and retroperitoneal
bleeding in abdominal cavity due to coagulopathy, or in tamponade of
non-surgical bleeding in subphrenic pelvic or retroperitoneal space, or
accumulation of blood coagula, but also in case of edema and leak of
intestinal wall from massive volume resuscitation and perfusion or in case
of tension closure of the abdominal cavity. ACS however develops also
after protracted abdominal cavity operations.
Clinical picture of developed ACS was probably defined best by
Ivatury in 1997, characterizing the abdominal distension, hypoxia and
hypercapnia with oliguria up to anuria, when this organ dysfunction is
adjusted only after performing the abdominal decompression [9].
With regard to the fact that abdominal compartment syndrome mostly shows
in polytraumatised patients in critical condition it is complex to
diagnose it, but it is not difficult because the application of method of
measuring the intracystic pressure in the urinary bladder, which is a
simple and miniinvasive method, allows for monitoring the intraabdominal
hypertension that fully corresponds with the intracystic pressure values.
Normal values of intraabdominal pressure range from 0-5 mmHg.
Slightly increased values are reported ranging from 10 to 15 mmHg,
when the heart index is usually maintained and renal symptoms do not
appear. However, with medium-increased values of 15-25 mmHg full abdominal
compartment symptom may already develop and if the organism fails to
respond to aggressive supply of fluids to the blood circulation with
temporary use of vasoconstriction means, it is recommended to carry out
the decompression operation of abdominal cavity, which is fully indicated
with IAP exceeding 25 mmHg [2].
From 1999 to 2002, 436 polytrauma patients were treated at the
Traumatological Centre of the University Hospital in Ostrava. Traffic
accident trauma prevailed in 73% together with sporting and leisure time
injuries. There were 87 abdominal cavity trauma, in this 31 injuries of
liver, 35 injuries of lien, 4 injuries of pancreas, 12 injuries of
entrails, and 5 injuries of retroperitoneum.
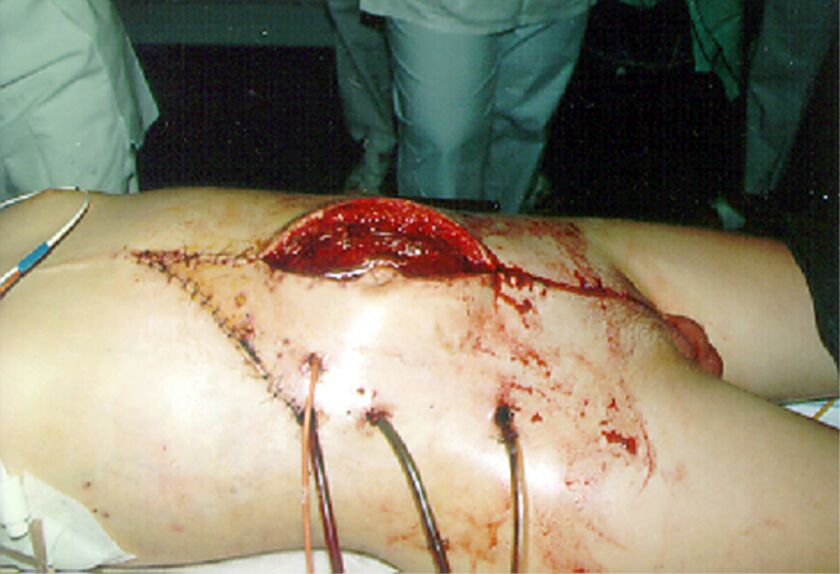
On
decompression laparotomy, 1500 ml of blood was found coming from the
retroperitoneal space, where revision found no surgical source of
bleeding; therefore, retroperitoneal tamponade was carried out and the
laparotomy was closed by plastic foil (Figure 2). The tamponade was
removed after 24 hours with definite closure of abdominal cavity in 7
days. The patient was dismissed for home treatment on 21st day.

Obr.
1
Discussion
Abdominal compartment syndrome has been indicated as complication in
serious abdominal trauma for more than 50 years. It develops as a
consequence of increased intraabdominal pressure not only in abdominal
trauma, but also in intestinal obstructions with serous edema of entrails
or chronically growing ascitus, in acute haemorrhagic necrotic
pancreatitis and septic peritonitis. In recent years, it occurrence has
been reported also in protracted operations in abdominal cavity with
subsequent extensive resuscitation [10].
The
increase of intraabdominal pressure is, however, also contributed to by
increased abdominal content on tamponade of non-surgical bleeding in
subphrenic, pelvic and retroperitoneal area, accumulation of blood
coagula, or possibly continued bleeding in abdominal cavity on
coagulopathy or on intestinal distension after injury of mesenterial
vessels, but, last but not least, also upon closure of abdominal cavity
under tension [11]. Progressively growing intraabdominal hypertension
always deteriorates the function of adjacent and distant organs, showing
in cardiovascular system by decreased minute cardiac volume as a
consequence of increased vascular resistance with decreased venous return
[20], which manifests by increased intrathoracic pressure with ventilation
and perfusion changes, hypoventilation, hypoxia and hypercapnia, and
decreased pulmonary compliance [19], the resulting condition of which is
restriction respiratory syndrome. Renal dysfunction is manifested by
oliguria up to anuria and develops based on decreased perfusion of
retroperitoneal, but also intraabdominal organs, when the solanchnic
ischemia affect not only the liver metabolism [6], but allows also for
translocation of endotoxins and bacteria through ischemized intestinal
mucous barrier, which allows for activation of septic syndrome trigger
factor [5]. Intraabdominal hypertension further causes also the increase
of intracranial pressure [2] with danger of ischemic neural damage with
decrease of cerebral perfusion pressure. All symptoms of these organ
dysfunctions are caused by acute increase of intraabdominal pressure with
consequences of abdominal compartment syndrome.
Clinical picture of ACS is characterised by abdominal distension, hypoxia
and hypercapnia with oliguria up to anuria, when the organ dysfunction
occurs after abdominal decompression. Persisting increase of
intraabdominal pressure over 25mmHg with clinical symptoms of ACS are the
indications for decompression operation of abdominal cavity.
During decompression operation, blood, blood coagula
and secreta are removed from the abdominal cavity. In the event of
continued non-surgical bleeding a tamponade is applied, which is
subsequently renewed, or the bleeding is treated surgically (wiring,
punch) and the abdominal cavity is flushed with warm saline [10].
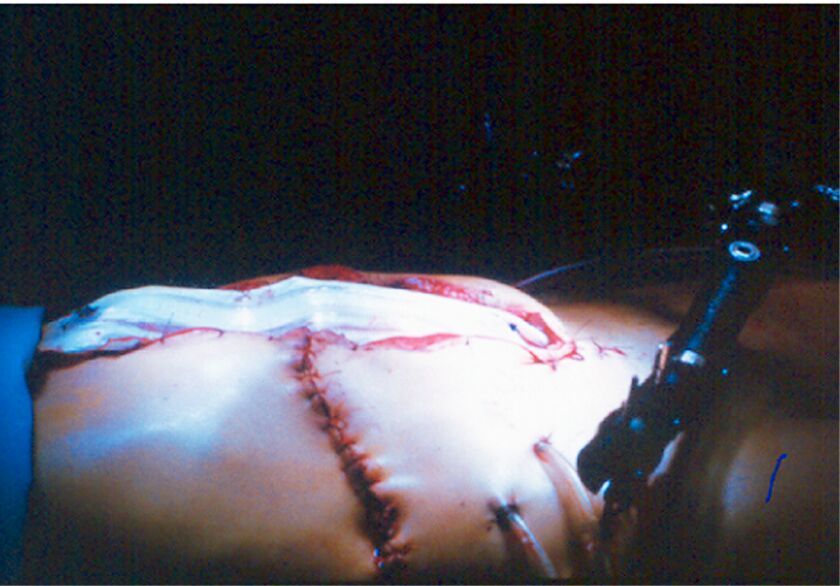
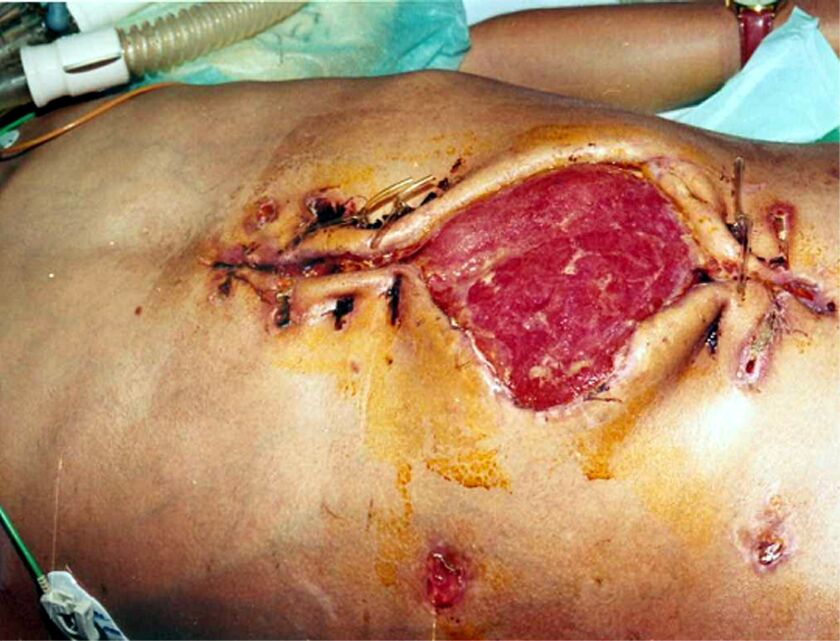
Laparotomy or relapatotomy is closed by means of synthetic material
– absorbable, non-absorbable mesh, plastic foil (Figure 3) and in recent
year also Ethizip.
Obr.
3
On every future revision of the abdominal cavity the
foil incision or release of Ethizip will be sufficient. In ideal case, we
can definitely close the abdominal revision after the last revision. In
the event of persisting defect of abdominal wall, ventral hernia may
develop, which will be treated in the second period (Figures 4, 5, 6).

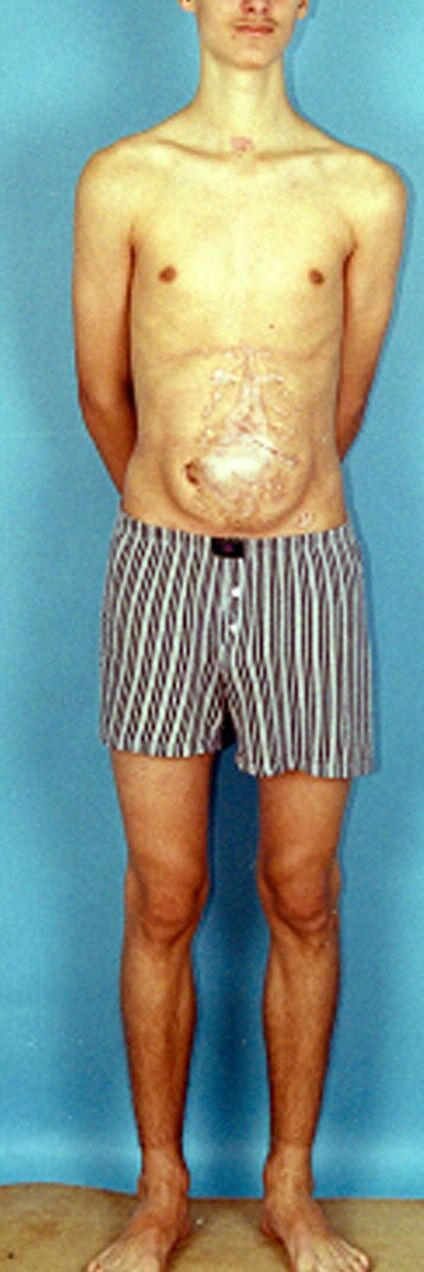
Fig 5
Fig 6
However, during or immediately after decompression
laparotomy symptoms of reperfusion syndrome may develop in come patients,
resulting even in asystolia caused, according to some authors, by sudden
decrease of system vascular resistance with subsequent serious hypovolemia
[13] or perfusion of anaerobic metabolism products from splanchnic area.
As a prevention to this complication, volume preliminary filling of the
circulation is recommended by application of 2 l of saline with Manitol
and bicarbonate applied immediately before decompression of abdominal
cavity [8].
In recent year, the literature has provided also preventive procedure to
prevent from ACS development, for which the patient endangered by ACS has
been defined. It is an
“abdominal catastrophe” patient in danger of bleeding to death,
treated by staged laparotomy method, often with tamponade, who has
received a large number of blood transfers with significant volume
therapy.
In these patients it is recommended to perform
preventive closure of primary laparotomy using the meshes or plastic
foils, which successfully prevents from development of ACS [13]. Primary
laparotomy closed with mesh or foil or Ethizip, as appropriate, allows for
faster abdominal cavity decompression in the event of increasing IAP event
in the ICU room, which prevents from further risk of complications
occurring during transport of the patient to the operating room, which
relates to the necessary ventilation support as most transport ventilators
do not achieve the necessary efficiency to maintain the adequate
respiratory volume in the event of increased respiratory pressures [8].
However, it is still impossible to specify fixed uniform criteria for
preventive use of temporary closure of abdominal cavity using the mesh or
foil, because it will always depend on subjective assessment of the
operator regarding the tension of abdominal cavity after proximation of
the fascia edges and estimation of the amount by which the content of
abdominal cavity may increase or has already increased during tamponade.
Further, however, there is a question whether it is not
more advantageous in hazard patient to carry out the primary closure of
abdominal cavity with post-operation IAP monitoring and early ACS
diagnostics instead of preventive temporary laparostomy.
Conclusion
Abdominal compartment syndrome is a serious multidiscipline issue of
urgent surgery, which the physicians must always be aware of in case of
any serious abdominal cavity trauma connected with massive bleeding, but
also in case of any protracted operation with massive volume resuscitation
including early post-operation periods. In the event of any suspicion for
acute elevation of intraabdominal pressure in these patients it is
essential to measure the intracystic pressure continuously, and in the
event of clinical symptoms of acute abdominal compartment syndrome with
increase of intracystic pressure over 25 mmHg the performance of
decompression laparotomy is indicated even with the assumption of negative
peroperation finding, with temporary closure of the abdominal cavity with
sterile foil or Ethizip. Therefore, acute abdominal compartment syndrome
is an abdominal emergency with urgent necessity to perform the early
decompression laparostomy to prevent from development of multiorgan
failure of the organism. There should be no indication hesitation to
perform the laparotomy even though abnormal coagulation parameters may
occur, because the acute decompression laparotomy reduces UAP and will
allow for tamponade with better compression of the bleeding surface, or it
may discover major bleeding, which can be treated surgically, but first of
all it will improve the mucous perfusion with acidosis reduction.
Therefore, acute decompression or reexploration of the abdominal cavity is
fully indicated n case of progressive growth f IAP or event abnormal
coagulation parameter [10].
References
1. BACKER, D. Abdominal compartment syndrome. Crit Care. 3, 1999, 6, s. 103–104.
2. BLOOMFIELD, G.L., DALTON, J.M., SUGERMAN, H.J. et al. Treatment of increasing intracranial pressure secondary to the acute abdominal compartment syndrome in patient with combined abdominal and head trauma. J Trauma. 39, 1995, 6, 1168–1170.
3. CARRY, P.Y. La pression intra-abdominal. Ann Fr Anesth Reanim. 13, 1994, 3, s. 381–389.
4. CULLEN, D.J., COYLE, J.P., TEPLICK, R. et al. Cardiovascular, pulmonary and renal effects of masively increased intra-abdominal pressure in critically ill patients. Crit Care Med. 17, 1989, 2, s. 118–121.
5. DIEBEL, L.N, DULCHAVSKY, S.A, WILSON, R.F. Effect of increased intra-abdominal pressure on mesenteric arterial and intestinal mucosal blood flow. J Trauma. 33, 1992, 1, s. 45–49.
6. DIEBEL, L.N., WILSON, R.F., DULCHAVSKY, S.A. et al. Effect of increased intra-abdominal pressure on hepatic arterial, portal venous, and hepatic microcirculatory blood flow. J Trauma. 33, 1992, 2, 279–282.
7. DIEBEL, L.N., WILSON, R.F., DULCHAVSKY, S.A. Effect of intra-abdominal pressure on abdominal wall blood flow. Am surg. 58, 1992, 9, s. 573–575.
8. EDDY, V., NUNN, C., MORRIS, J.A. Abdominal compartment syndrome. Surg Clin Am. 77, 1997, 8, s. 801–812.
9. IVATURY, R.R., DIEBEL, L., PORTER, J.M. et al. Intra-abdominal hypertension and the abdominal compartment syndrome. Surg Clin Am. 77, 1997, 4, s. 783–800.
10. IVATURY, R.R., PORTER, J.M., SIMON, R.J. et al. Intra-abdominal hypertension after life-threatening penetrating abdominal trauma: Prophylaxis, Incidence, and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J Trauma. 44, 1998, 6, s. 1016–1021.
11. IVATURY, R.R., SIMON, J. Intra-abdominla hypertension: the abdominal compartment syndrome. Crit Care. 73, 1996, 951.
12.
IVATURY, R.R, Schein,
M. Intraabdominal hypertension and the abdominal compartment syndrome. Br
J Surg. 85, 1998, 8, s. 1027–1028.
13. KITKA, M., PLEVA, L. Poranenia orgánov brušnej dutiny. Košice : Klinika úrazovej chirurgie LF UPJŠ a FNLP, 2003. 1. vyd. 73 s.
14. KRON, I. L., HARMANN, P. K., NOLAN, S. P. The Measurement of Intra-abdominal Pressure as a Criterion for Abdominal Re-exploration. Ann Surg. 1999, 1984, 1, 28–30.
15. MAŠEK, M., ŽÁK, J., CHALUPNÍK, Š., ŠRÁMEK, V. Nejčastější chyby v měření nitrobřišního tlaku. Úraz chir. 11, 2003, 1, s. 18–21.
16. McQUEEN, GASTON, P., COURT-BROWN, C.M. Acute compartment syndrome. J Bone Surg. 82-B, 2000, 3, s. 200–203.
17. MICHEK, J., PLEVA, L., WENDSCHE, P. Poranění orgánů dutiny břišní a retroperitonea. Ostrava : Cicero, 1. vyd. 2001, 134 s.
18. MOORIS, J.A, EDDY, V.A, BLINMAN, T.A. et al. The staged celiotomy for trauma. Ann Surg. 217, 1993, s. 576–586.
19. OBEID, F., FATH, J., GUSLITS, B. et al. Increases in intraabdominal pressrue affect pulmonary compliance. Arch Surg. 130, 1995, 5, s. 544–548.
20. RIDINGS, P.C., BLOOMFIELD, G.L., BLOCHER, Ch.R. et al. Cardiopulmonaly effects of raised intra-abdominal pressure before and after intravascular volume expansion. J Trauma. 39, 1995, 6, s. 1071–1075.
21. SURGUE, M. Intra-abdominal pressure. Clin Intensiv Care. 6, 1995, 2, s. 76–79.
22. ZELENAK, J. et al. Injuries of the intraabdominal organs at patients with polytrauma. Bratisl Lék Listy. 104, 2003, 2, s. 82–86.
Doc. MUDr. Leopold Pleva, CSc.
Gen. Hrušky 4
703 00 Ostrava-Mar. Hory